Doh 4359 Form Printable
Doh 4359 Form Printable - Hit done and download the filled out form to. Web doh 4359 form printable. Web complete doh 4359 2020 online with us legal forms. Web complete doh 4359 printable form online with us legal forms. Save or instantly send your ready documents. Web send doh 4359 via email, link, or fax. Edit your doh 4359 template online. Web get your doh 4359 form in 3 easy steps. Get everything done in minutes. Web the guide of completing doh 4359 printable online.

Doh 4359 Fill Online, Printable, Fillable, Blank pdfFiller
If you are looking about alter and create a doh 4359 printable, here are the easy guide you need to follow: Type text, add images, blackout confidential details,. Web the guide of completing doh 4359 printable online. Tips on how to accurately. 01 fill and edit template.
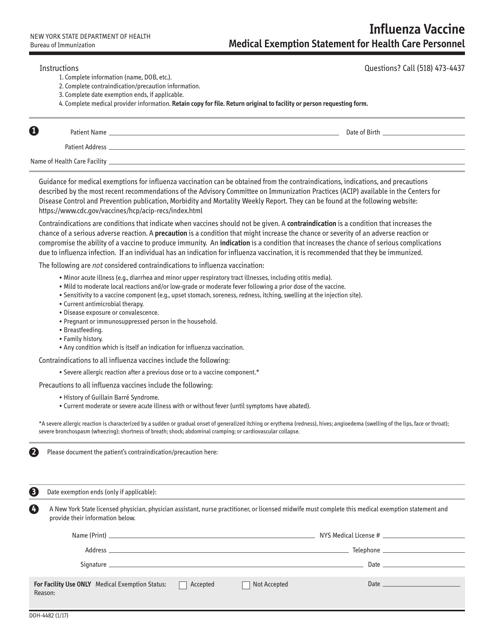
Form DOH4482 Download Printable PDF or Fill Online Influenza Vaccine
Easily fill out pdf blank, edit, and sign them. Edit your doh 4359 template online. Get everything done in minutes. Web complete doh 4359 2020 online with us legal forms. Get everything done in minutes.
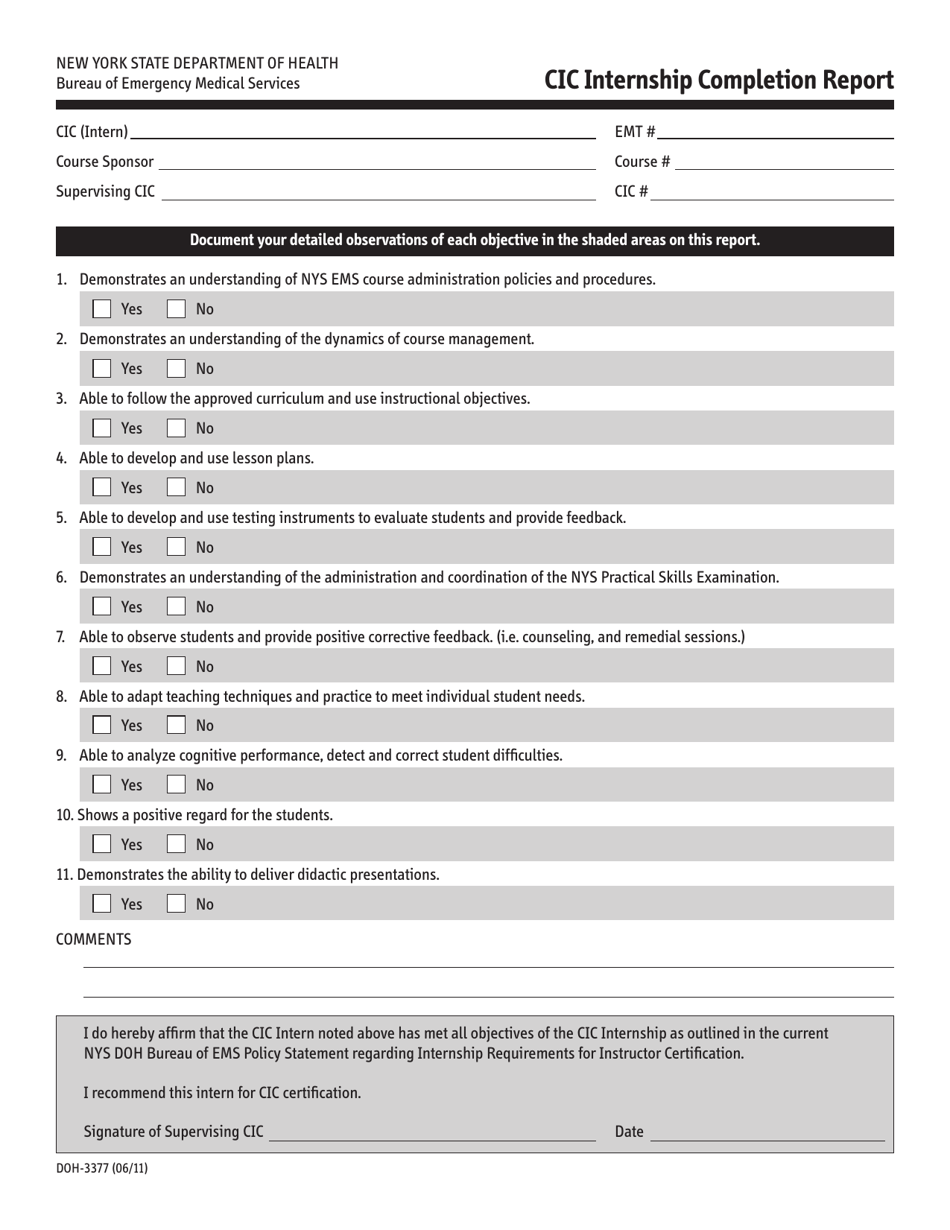
Form DOH3377 Download Printable PDF or Fill Online Cic Internship
Web doh 4359 form printable. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. Web are you considering to get doh 4359 form to fill? 01 fill and edit template. Check out how easy it is to complete and esign documents online using fillable.

Doh 4469 form financial status Fill out & sign online DocHub
Patient identifying information (use additional paper if necessary) patient name cin date of birth sex address: Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Get everything done in minutes. You can also download it, export it or print it out. Easily fill out pdf blank, edit, and sign them.
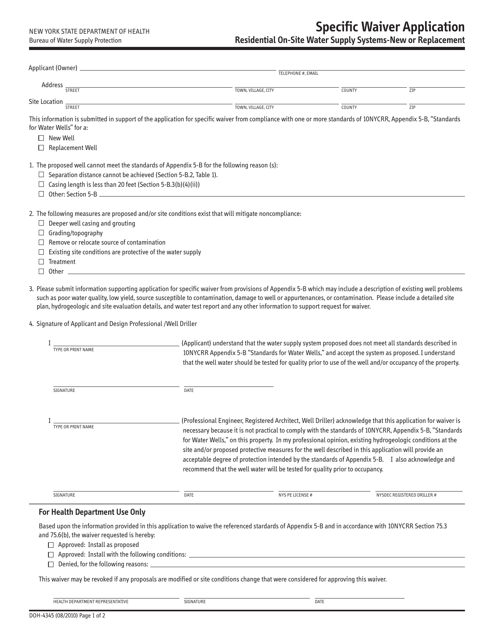
Form DOH4345 Download Printable PDF or Fill Online Specific Waiver
Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web get your doh 4359 form in 3 easy steps. Indicate n/a if an item does not apply to this patient or unk if the.
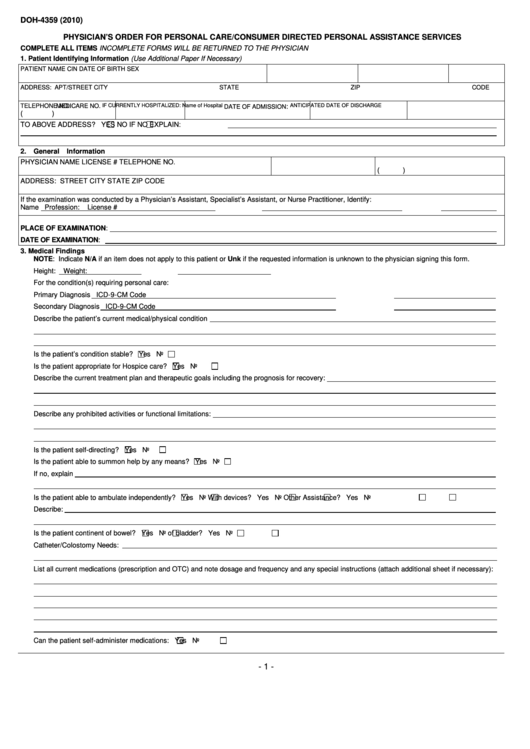
Fillable Doh 4359 (2010) Physician'S Order For Personal Care/consumer
Edit your doh 4359 template online. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Save or instantly send your ready documents. Web doh 4359 form printable. Web send doh 4359 via email, link, or fax.

Doh 102 Form Fill Online, Printable, Fillable, Blank pdfFiller
Web get your doh 4359 form in 3 easy steps. Easily fill out pdf blank, edit, and sign them. Easily fill out pdf blank, edit, and sign them. 03 export or print immediately. Tips on how to accurately.
Download Fillable da Form 4359
Web send doh 4359 via email, link, or fax. Hit done and download the filled out form to. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web are you considering to get doh 4359 form to fill? Web complete doh 4359 2020 online with us legal forms.

Fill DOH4359 (2010) PHYSICIANS ORDER FOR PERSONAL CARECONSUMER DIRECTED
Get everything done in minutes. If you are looking about alter and create a doh 4359 printable, here are the easy guide you need to follow: Web complete doh 4359 2020 online with us legal forms. Edit your doh 4359 template online. Web send doh 4359 via email, link, or fax.
Doh Application Form for Renewal of License to Operate Fill Out and
Look through the entire template to make sure you?ve filled in all the information and no changes are needed. Easily fill out pdf blank, edit, and sign them. If you are looking about alter and create a doh 4359 printable, here are the easy guide you need to follow: Save or instantly send your ready documents. Web are you considering.
The best place to get access to and. Save or instantly send your ready documents. Web doh 4359 form printable. Web complete doh 4359 2020 online with us legal forms. You can also download it, export it or print it out. Web the guide of completing doh 4359 printable online. Web get your doh 4359 form in 3 easy steps. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Easily fill out pdf blank, edit, and sign them. Easily fill out pdf blank, edit, and sign them. Get everything done in minutes. Get everything done in minutes. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. Web complete doh 4359 printable form online with us legal forms. Web send doh 4359 via email, link, or fax. Apt/street city zip code state telephone. Patient identifying information (use additional paper if necessary) patient name cin date of birth sex address: Look through the entire template to make sure you?ve filled in all the information and no changes are needed. 01 fill and edit template.