Printable Medical Records Release Form
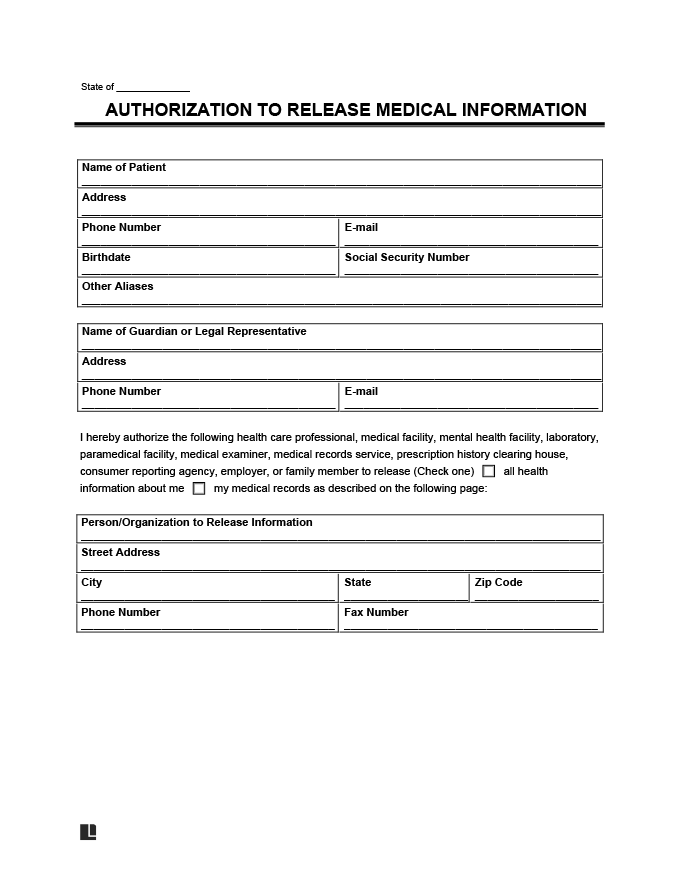
Printable Medical Records Release Form - You can use one of our free printable templates (pdf & word) to authorize the. Web release my medical records from **check one option allina health (optional: To fill out a hipaa release form, a patient must choose the appropriate document. Send or bring the completed form to the subject of the record's local. Web medical release forms are used to request that a healthcare provider share a patient’s medical history with a third party (employer, insurance company, school, etc.). If specific dates only, list dates:. Web a consent form that includes a request for medical records is valid for 90 days from the date of signature. Medical records release form sample. Lawdepot.com has been visited by 100k+ users in the past month This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an.
Medical Records Release (HIPAA) Form PDF & Word Legal Templates
Lawdepot.com has been visited by 100k+ users in the past month If any sections are left blank, this form will be invalid and it will not be possible for your health. Send or bring the completed form to the subject of the record's local. Download free version (pdf format) download editable. Web complete and submit the appropriate authorization form below:
Medical Records Release Form templates free printable
Lawdepot.com has been visited by 100k+ users in the past month The form must allow them to request their personal health information (phi) or grant a third party permission to release it. Web a patient can consent to the release of health information with this health information release authorization form. Web use the links above to access, print, and complete.

Medical Record Release Form Templates in 2021 Medical record, Medical
Web complete and submit the appropriate authorization form below: Web release my medical records from **check one option allina health (optional: Lawdepot.com has been visited by 100k+ users in the past month This includes specific permission to release: This form is to be used by a patient or legal representative to authorize the release of information to a third party.

Download New York Medical Records Release Form 1 for Free TidyTemplates
Download free version (pdf format) download editable. Web use the links above to access, print, and complete the authorization form. Web a patient can consent to the release of health information with this health information release authorization form. Web a medical records release form is used to request that a health care provider (physician, dentist, hospital, chiropractor, psychiatrist, etc.) release.
FREE 12+ Sample Medical Records Release Forms in PDF MS Word Excel
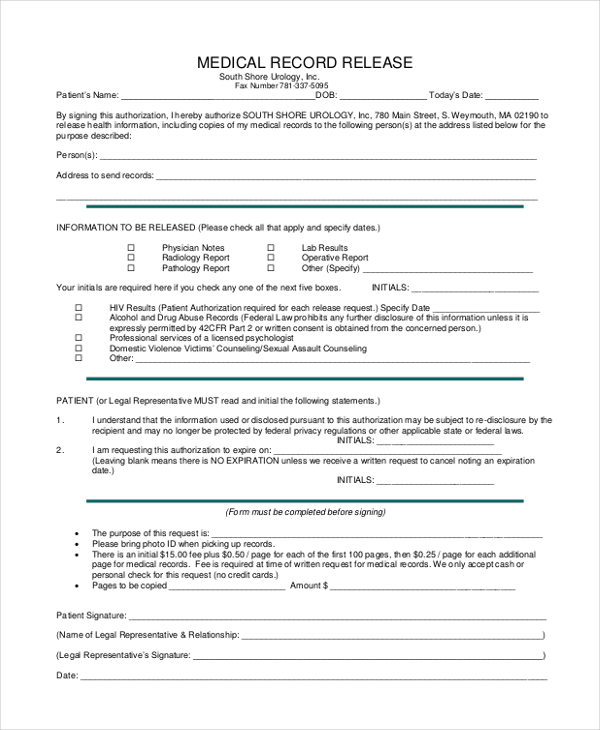
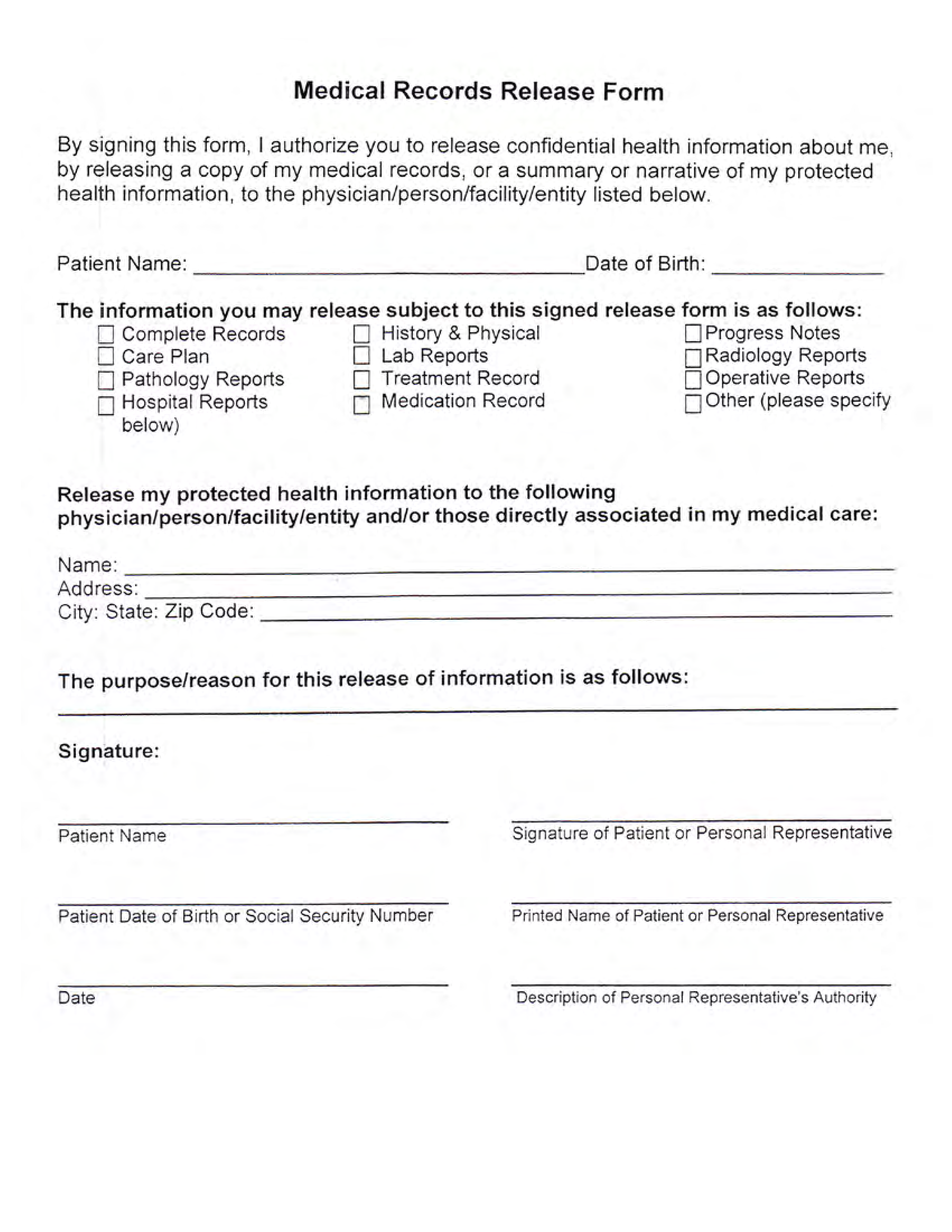
Web patient’s name (print) phone number date of birth patient’s address medical record # information that can be released: You can use one of our free printable templates (pdf & word) to authorize the. Web hipaa release form please complete all sections of this hipaa release form. Specify location or provider below): Web release my medical records from **check one.
Medical Records Release Form Templates at
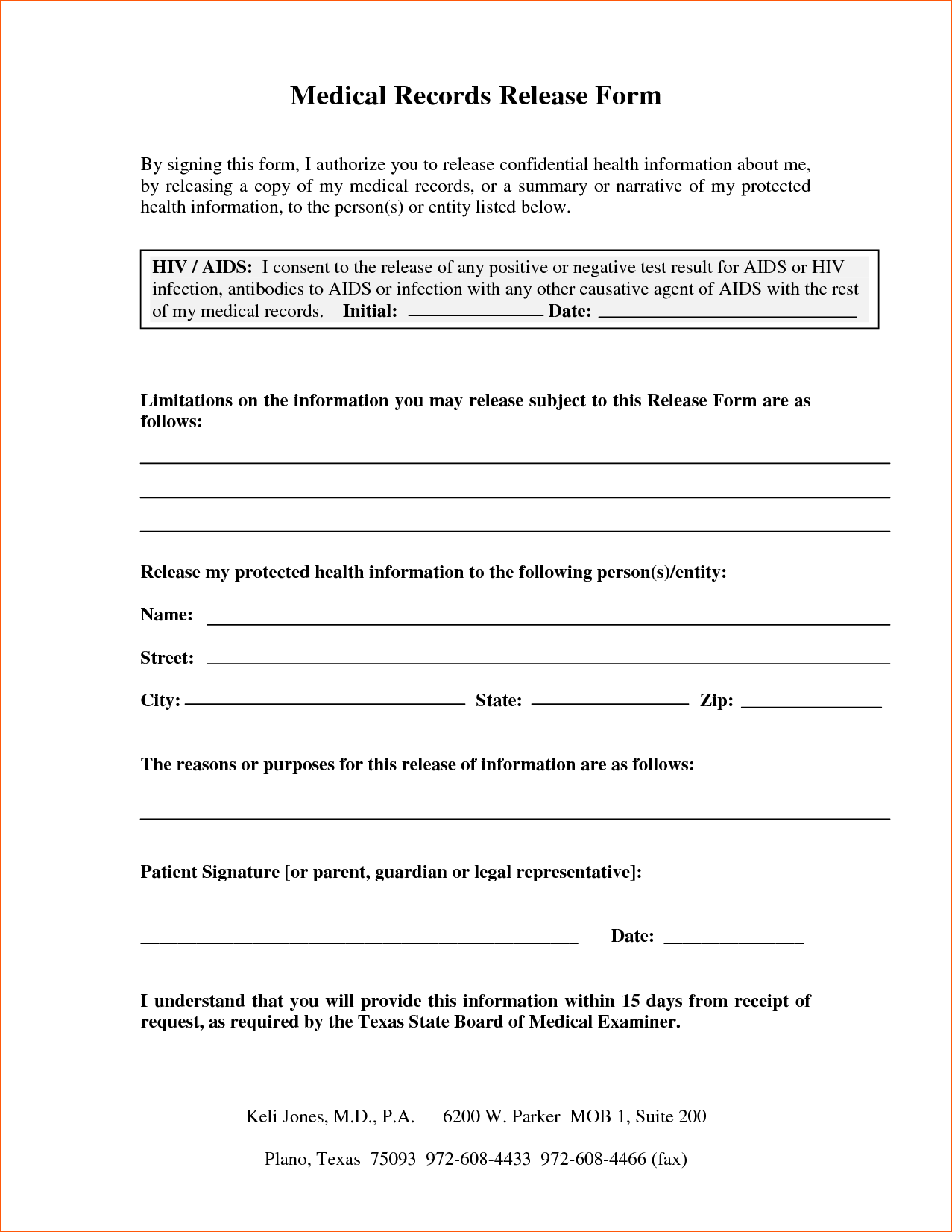
Web a patient can consent to the release of health information with this health information release authorization form. Web a medical records release form is used to request that a health care provider (physician, dentist, hospital, chiropractor, psychiatrist, etc.) release a patient's medical records,. Medical records release form sample. This form is to be used by a patient or legal.
Medical Release Form Fill Online, Printable, Fillable, Blank pdfFiller
If specific dates only, list dates:. Also education records and other information related to my ability to perform tasks. Web complete and submit the appropriate authorization form below: Lawdepot.com has been visited by 100k+ users in the past month Send or bring the completed form to the subject of the record's local.

Free Medical Release Form Template Continuum
Web all my medical records: This includes specific permission to release: To fill out a hipaa release form, a patient must choose the appropriate document. Specify location or provider below): If specific dates only, list dates:.
Generic Medical Records Release Form download free documents for PDF
This includes specific permission to release: If specific dates only, list dates:. Web a patient can consent to the release of health information with this health information release authorization form. The form must allow them to request their personal health information (phi) or grant a third party permission to release it. Web hipaa release form please complete all sections of.
4 Best Images of Free Printable Medical Release Forms Car Accident
Web patient’s name (print) phone number date of birth patient’s address medical record # information that can be released: Web creating your own account gives you 24/7 access to a select set of medical records. Request your records or information from your upmc physician office. If any sections are left blank, this form will be invalid and it will not.
If any sections are left blank, this form will be invalid and it will not be possible for your health. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Web hipaa release form please complete all sections of this hipaa release form. Web complete and submit the appropriate authorization form below: Web a patient can consent to the release of health information with this health information release authorization form. Web use the links above to access, print, and complete the authorization form. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize. Send or bring the completed form to the subject of the record's local. Web complete a medical records release form. 7100 west center rd, omaha, ne 68106. Web a medical records release form is used to request that a health care provider (physician, dentist, hospital, chiropractor, psychiatrist, etc.) release a patient's medical records,. Request your records or information from your upmc physician office. Web may 17, 2022 by printablee printable medical release form template printable medical release forms how to get a medical release form? Uslegalforms.com has been visited by 100k+ users in the past month Web care everywhere medical and billing record release forms use these forms when requesting transfer of your medical and billing records to or from another provider or to. You can use one of our free printable templates (pdf & word) to authorize the. This includes specific permission to release: Web a consent form that includes a request for medical records is valid for 90 days from the date of signature. Web all my medical records: Authorization to disclose protected health information to family and friends adult patient.